There are a number of approaches to studying medication-taking behavior. Self-report measures have the benefits of being cheap, easy to administer, non-intrusive, and able to provide information on attitudes and beliefs about medication. Potential limitations to self-report are that the ability to understand the items, and willingness to disclose information, can affect response accuracy and, thus, questionnaire validity. Among the various self-report scales for measuring adherence to medication, 8-items Morisky scale is widely used nowadays. However, I am going to talk about other scale other than 8-items Morisky scale.
1. The Summary of Diabetes Self-Care Activities Measure
The SDSCA measure is a brief self-report questionnaire of diabetes self-management that includes items assessing the following aspects of the diabetes regimen: general diet, specific diet, exercise, blood-glucose testing, foot care, and smoking. Normative data (means and SD), inter-item and test-retest reliability, correlations between the SDSCA subscales and a range of criterion measures, and sensitivity to change scores are presented for the 7 different studies (5 randomized interventions and 2 observational studies).
Participants were typically older patients, having type 2 diabetes for a number of years, with a slight preponderance of women. The average inter-item correlations within scales were high (mean = 0.47), with the exception of specific diet; test-retest correlations were moderate (mean = 0.40). Correlations with other measures of diet and exercise generally supported the validity of the SDSCA subscales (mean = 0.23). [Toobert DJ et.al]
• Weakness and strength.
There are numerous benefits from standardization of measures across studies. The SDSCA questionnaire is a brief yet reliable and valid self-report measure of diabetes self-management that is useful both for research and practice. The revised version and its scoring are presented, and the inclusion of this measure in studies of diabetes self-management is recommended when appropriate.
The inconsistent number of questionnaire items and constructs in each of the 7 studies constitutes a weakness of this analysis. However, in spite of shifting numbers of items and constructs throughout the 18 years of research with this instrument, the validity and reliability are remarkably stable.
• Degree for their use in research purpose
The use of this tool in research purpose is significantly increasing in the diabetes patients in all the county including the developing country like Ethiopia. [hailu.et.al]
• Should there be change pertaining to inter-cultural differences?
For the cultural adaptation, many researchers translated the English version of the tool to their native language. The term “cross-cultural adaptation” is used to encompass a process that looks at both language (translation) and cultural adaptation issues in the process of preparing a questionnaire for use in another setting.
In some cases, this is more obvious than in others. Guillemin et al suggest five different examples of when attention should be paid to this adaptation by comparing the target (where it is going to be used) and source (where it was developed) language and culture. The first scenario is that it is to be used in the same language and culture in which it was developed. No adaptation is necessary. The last scenario is the opposite extreme, the application of a questionnaire in a different culture, language and country [beaten et.al].
The Summary of Diabetes Self-Care Activities
The questions below ask you about your diabetes self-care activities during the past 7 days. If you were sick during the past 7 days, please think back to the last 7 days that you were not sick.
Diet
- How many of the last SEVEN DAYS have you followed a healthful eating plan?
0 1 2 3 4 5 6 7
- On average, over the past month, how many DAYS PER WEEK have you followed you’re eating plan?
0 1 2 3 4 5 6 7
- On how many of the last SEVEN DAYS did you eat five or more servings of fruits and vegetables?
0 1 2 3 4 5 6 7
- On how many of the last SEVEN DAYS did you eat high fat foods such as red meat or full-fat dairy products?
0 1 2 3 4 5 6 7
Exercise
- On how many of the last SEVEN DAYS did you participate in at least 30 minutes of physical activity? (Total minutes of continuous activity, including walking).
0 1 2 3 4 5 6 7
- On how many of the last SEVEN DAYS did you participate in a specific exercise session (such as swimming, walking, biking) other than what you do around the house or as part of your work?
0 1 2 3 4 5 6 7
Blood Sugar Testing
- On how many of the last SEVEN DAYS did you test your blood sugar?
0 1 2 3 4 5 6 7
- On how many of the last SEVEN DAYS did you test your blood sugar the number of times recommended by your health care provider?
0 1 2 3 4 5 6 7
Foot Care
- On how many of the last SEVEN DAYS did you check your feet?
0 1 2 3 4 5 6 7
- On how many of the last SEVEN DAYS did you inspect the inside of your shoes?
0 1 2 3 4 5 6 7
Smoking
- Have you smoked a cigarette—even one puff—during the past SEVEN DAYS?
0. No
1. Yes. If yes, how many cigarettes did you smoke on an average day?
Number of cigarettes:………………..
Self-Care Recommendations
1A. Which of the following has your health care team (doctor, nurse, dietitian, or diabetes educator) advised you to do?
Please check all that apply:
a. Follow a low-fat eating plan
b. Follow a complex carbohydrate diet
c. Reduce the number of calories you eat to lose weight
d. Eat lots of food high in dietary fiber
e. Eat lots (at least 5 servings per day) of fruits and vegetables
f. Eat very few sweets (for example: desserts, non-diet sodas, candy bars)
g. Other (specify):
h. I have not been given any advice about my diet by my health care team.
2A. Which of the following has your health care team (doctor, nurse, dietitian or diabetes educator) advised you to do?
Please check all that apply:
a. Get low level exercise (such as walking) on a daily basis.
b. Exercise continuously for a least 20 minutes at least 3 times a week.
c. Fit exercise into your daily routine (for example, take stairs instead of elevators, park a block away and walk, etc.)
d. Engage in a specific amount, type, duration and level of exercise.
e. Other (specify):
f. I have not been given any advice about exercise by my health care team.
3A. Which of the following has your health care team (doctor, nurse, dietitian, or diabetes educator) advised you to do?
Please check all that apply:
a. Test your blood sugar using a drop of blood from your finger and a color chart.
b. Test your blood sugar using a machine to read the results.
c. Test your urine for sugar.
d. Other (specify):
e. I have not been given any advice either about testing my blood or urine sugar level by my health care team.
4A. Which of the following medications for your diabetes has your doctor prescribed?
Please check all that apply.
a. An insulin shot 1 or 2 times a day.
b. An insulin shot 3 or more times a day.
c. Diabetes pills to control my blood sugar level.
d. Other (specify):
e. I have not been prescribed either insulin or pills for my diabetes.
Diet
5A. On how many of the last SEVEN DAYS did you space carbohydrates evenly through the day?
0 1 2 3 4 5 6 7
Medications
6A. On how many of the last SEVEN DAYS, did you take your recommended diabetes medication?
0 1 2 3 4 5 6 7
OR
7A. On how many of the last SEVEN DAYS did you take your recommended insulin injections?
0 1 2 3 4 5 6 7
8A. On how many of the last SEVEN DAYS did you take your recommended number of diabetes pills?
0 1 2 3 4 5 6 7
Foot Care
9A. On how many of the last SEVEN DAYS did you wash your feet?
0 1 2 3 4 5 6 7
10A. On how many of the last SEVEN DAYS did you soak your feet?
0 1 2 3 4 5 6 7
11A. On how many of the last SEVEN DAYS did you dry between your toes after washing?
0 1 2 3 4 5 6 7
Smoking
12A. At your last doctor’s visit, did anyone ask about your smoking status?
0. No
1. Yes
13A. If you smoke, at your last doctor’s visit, did anyone counsel you about stopping smoking or offer to refer you to a stop-smoking program?
0. No
1. Yes
2. Do not smoke.
14A. When did you last smoke a cigarette?
- More than two years ago, or never smoked
- One to two years ago
- Four to twelve months ago
- One to three months ago
- Within the last month
- Today
Scoring Instructions for the Summary of Diabetes Self-Care Activities
Scores are calculated for each of the five regimen areas assessed by the SDSCA: Diet, Exercise, Blood-Glucose Testing, Foot- Care, and Smoking Status.
Step 1:
For items 1–10, use the number of days per week on a scale of 0–7. Note that this response scale will not allow for direct comparison with the percentages.
Step 2: Scoring Scales
- General Diet = Mean number of days for items 1 and 2.
- Specific Diet = Mean number of days for items 3, and 4, reversing item 4 (0=7, 1=6, 2=5, 3=4, 4=3, 5=2, 6=1, 7=0).
Given the low inter-item correlations for this scale, using the individual items is recommended.
- Exercise = Mean number of days for items 5 and 6.
- Blood-Glucose Testing = Mean number of days for items 7 and 8.
- Foot-Care = Mean number of days for items 9 and 10.
- Smoking Status = Item 11 (0 = nonsmoker, 1 = smoker), and number of cigarettes smoked per day.
2. Brief Medication Questionnaire (BMQ)
Brief Medication Questionnaire (BMQ) is a self-report tool for screening adherence and barriers to adherence. It has three main question headings and multiple sub questions. The tool includes:
- a 5-item Regimen Screen that asks the patients about their medications that they were currently taking. Questions are asked to list the name of each medication, frequency of medication per day, number of days and times they have received each medication along with the number of times the patient missed taking medications in the past week,
- a 2-item Belief Screen consists of two questions that ask the patients whether they had any difficulty with any of the medications, and does the medication bother them in any way,
- a 2-item Recall Screen assesses the patient’s difficulty in recalling and remembering the dosage regimen of their medications, and
- a 2-item Access screen that evaluates the patient difficulty in buying and refilling their medications in time.
This method was applied in the cross-sectional study of hypertensive people enrolled at least six months in the program to assist hypertensive and diabetic individuals, provided in Brazil. The analysis of BMQ in this study showed that the regimen screen performed better than the other screens and the Medication Adherence Questionnaire (MAQ) for the identification of low adherence among people with uncontrolled hypertension..
BMQ regimen screen which was strongly associated with control of blood pressure. From the point of view of program planning in public health, such evaluation can indicate which patients should receive educational reinforcement, pharmaceutical support and multidisciplinary care and which require adjustment of therapeutic regimens. Evaluation of adherence may help clinicians discriminate between inadequate use of medication and insufficient treatment regimen.
3. The Hill-Bone Compliance Scale
The Hill-Bone Compliance Scale addresses barriers and self-efficacy but are limited in their generalizability. The Hill Bone Compliance Scale focuses on hypertensive patients. This scale assesses patient behaviors for three important behavioral domains of high blood pressure treatment:
1) reduced sodium intake;
2) appointment keeping; and
3) medication taking.
This scale is comprised of 14 items in three subscales. Each item is a four point Likert type scale. The content validity of the scale was assessed by a relevant literature review and an expert panel, which focused on cultural sensitivity and appropriateness of the instrument for low literacy.
This scale was validated in most investigations, among others for use in a South African primary health care setting, because hypertension is prevalent, under-diagnosed, and inadequately treated in Black South Africans. The authors demonstrated criterion validity and internal consistency for a modified Hill-Bone. Results compare favorably with those from an urban African-American setting (standardized Cronbach alpha was 0.74–0.84). This study demonstrates that many of the behavioral aspects of the fundamental elements of high blood pressure care and control, such as the medication taking, appointment keeping, and salt intake reduction, are measurable across cultures. Second, the study showed that vigorous psychometric methods can be used effectively in different cultural groups. Third, the study demonstrates that both concurrent and predictive validity can be assessed quickly in a clinical setting. In cases of insufficiently controlled blood pressure, it is important for practitioners to distinguish between »nonadherence« and »nonresponse« to antihypertensive drug treatment. A reliable and valid adherence measurement based on the patient’s self-report may be helpful in daily practice.
In a primary care sample with 353 hypertensive patients, the authors applied two self-rating instruments to assess medication adherence (the »Hill-Bone Compliance to High Blood Pressure Therapy Scale« and Morisky’s »Self-Reported Measure of Medication Adherence«) and comparing their psychometric properties. The use of both scales cannot be recommended. They showed considerable floor effects, and their ability to identify medication adherence was inconsistent for nearly every third patient. The power of both scales to predict uncontrolled blood pressure was essentially a chance. The underlying conceptual framework of medication adherence therefore needs to be rethought.

4. The Medication Adherence Rating Scale (MARS)
Adherence to medication is an important predictor of illness course and outcome in psychosis. The Medication Adherence Rating Scale (MARS) was developed from Morisky et al’s Medication Adherence Questionnaire (MAQ), is a ten-item self-report measure of medication adherence in psychosis. To summarize, theMARS is a quick, non-intrusive measure of medication adherence. Its reliability is adequate, but validity appears only moderate-weak. Items in the MARS about attitude to medication may be informative to clinicians identifying barriers to adherence in individual cases, but do not appear to be valuable in predicting adherence behavior over a large sample. Factor 1 (medication adherence behavior), corresponding to the Medication Adherence Questionnaire (MAQ), may be superior for this purpose. The MARS total score reproduced the expected relationships of higher adherence with more insight into the need for medication, and higher adherence with less psychopathology.

5. Morisky Green Levine Scale
Four-item MGLS, which includes four questions with yes/no response options. The MGLS results in a score ranging from 0 to 4, and the developers suggested three levels of medication adherence on the basis of this score: high, medium, and low adherence with 0, 1 to 2, and 3 to 4 points, respectively. A dichotomous definition of adherence on the basis of the MGLS is also commonly used, with 0 points indicating perfect adherence and 1+ point indicating some level of non-adherence.
Morisky Green Levine Test
"Yes" item(s) Interpretation
0= High adherence
1 or 2=Medium adherence
3 or 4=Low adherence
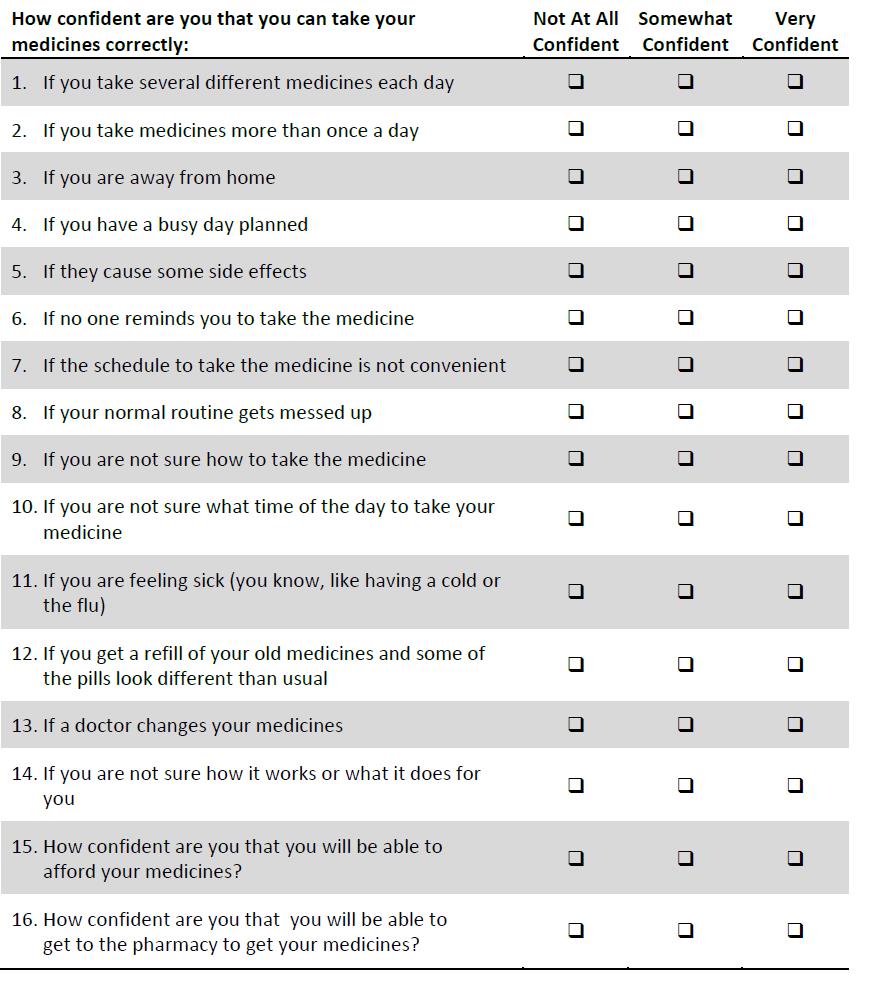
6. Self-efficacy for Appropriate Medication Use (SEAMS)
The Self-efficacy for Appropriate Medication Use (SEAMS) was developed by a multidisciplinary team with expertise in medication adherence and health literacy. Its psychometric properties were evaluated among 436 patients with coronary heart disease and other comorbid conditions. Reliability was evaluated by measuring internal consistency and test-retest reliability. The final 13-item scale had good internal consistency reliability (Cronbach’s alpha=0.89). The SEAMS is a reliable and valid instrument that may provide a valuable assessment of medication self-efficacy in chronic disease management, and appears appropriate for use in patients with low literacy skills.
Because of poor adherence to oral osteoporosis medications, SEAMS was applied on five hundred women aged 55 years and older who were newly prescribed daily or weekly oral bisphosphonates, were randomly selected from Kaiser Permanente Southern California, a large integrated health care delivery system, and mailed a self-administered survey that included, among others, and SEAMS.
7. Adherence to Refills and Medications Scale (ARMS)
The Adherence to Refills and Medications scale (ARMS) was developed, pilot tested, and administered to 435 patients with coronary heart disease in an inner-city primary care clinic. Psychometric evaluation performed overall and by literacy level, included an assessment of internal consistency, test-retest reliability, and factor analysis. Criterion-related validity was evaluated by comparing scores with Morisky’s self-reported measure of adherence, medication refill adherence, and blood pressure measurements. Lexile analysis was performed to assess the reading difficulty of the instrument.
The final 12-item scale had high internal consistency overall (Cronbach’s alpha=0.814) and among patients with inadequate (alpha=0.792) or marginal/adequate literacy skills (alpha=0.828). Factor analysis yielded two subscales, which pertained to taking medica- tions as prescribed and refilling medications on schedule. The ARMS correlated significantly with the Morisky adherence scale (Spearman’s rho=–0.651, p<0.01), and it correlated more strongly with measures of refill adherence than did the Morisky scale. Patients with low ARMS scores (which indicated better adherence) were significantly more likely to have controlled diastolic blood pressure (p<0.05), and tended to have better systolic blood pressure control. Lexile analysis demonstrated that the instrument had a favorable reading difficulty level below the eight grades. The ARMS is a valid and reliable medication adherence scale when used in a chronic disease population, with good performance characteristics even among low-literacy patients.

8. Scale for measurement adherence to medication applied in Zagreb, Croatia
This scale was applied in the study that was designed as a cross-sectional survey by use of a self-administered 33-item questionnaire. The questionnaire listed 16 common reasons for nonadherence and study subjects had to answer questions on each of these reasons as the possible cause of his/her nonadherence. This final 16--item scale had good internal consistency reliability (Cronbach’s alpha=0.89)24. These answers were used to analyze the impact of each of these reasons for nonadherence.
The study included 635 individuals collecting or buying drugs for the treatment of chronic diseases, with special reference to subjects taking antihypertensive agents (N=361). The survey was conducted at Zagreb (Croatia) pharmacies and the questionnaire was filled out by study subjects with instructions and help provided by the pharmacist as questionnaire administrator.
According to medication adherence, study subjects were divided into two groups of adherent and nonadherent subjects, as declared by themselves. The subjects answering the respective question that they had never failed to take their medication on time were considered as adherent, and all others as nonadherent subjects.

9. Adherence in Chronic Diseases Scale (ACDS)
The ACDS questionnaire, created by A. Kubica, was designed to examine chronically ill adult patients. It allows the assessment of adherence itself, as well as identification of the most important factors influencing adherence, such as: acceptance of a therapy plan, cooperation between a patient and health care professionals, and the economic status of a patient. The scale’s validation was performed in a group of 413 patients with coronary artery disease. Originally, the survey included eight questions with five possible answers. Four questions (No. 1, 3, 4, 5) concern the regularity of taking medications in prescribed doses, one question (No. 6) concerns acceptance of the provided therapy, while the last two questions (No. 7 and 8) refer to the patient-physician cooperation. The second question, referring to the assessment of the treatment-related financial burden, was finally removed due to insufficient cohesion with the other components of the questionnaire. The result is a sum of all gained points.
In the original version of ACDS, possible scores ranged from 0 to 32. Results below 24 points matched low adherence, while results of 24-28 points and above 29 points corresponded to medium and high adherence, respectively. The removal of the second question from the survey resulted in new centile distribution and reduced the spectrum of results to a range from 0 to 28 points. This time, results below 21 points, between 21–26 points, and above 26 points correspond, respectively, to low, medium, and high adherence. The internal consistency of the ACDS final version was assessed using Cronbach’s alpha coefficient, and the value of 0.752 confirmed high reliability and homogeneity of the questionnaire.
The scale is simple to use and may be applied in everyday medical practice and for research purposes. The ability to assess the attitudes and behavior of patients including the essential elements of the treatment process should be highlighted as strengths of this scale.. The ASCD is available for free on the website of the Faculty of Health Science of the Nicolaus Copernicus University, Collegium Medium

10. Martin-Bayarre-Grau Questionnaire(MBG)
The Martin-Bayarre-Grau, a Spanish language 12-item questionnaire, was validated in Cuba in a population of 114 hypertensive patients. The Cronbach’s alpha coefficient of internal consistency was 0.889 for the sample. The second validation was performed in 142 patients with hypertension, with a Cronbach’s alpha value of 0.694. Validation results showed that the formulation of items was reasonable, clearly defined, and justified. The validation procedures allowed recognition of the existence of three factors: active adherence, autonomy in the face of treatment, and adherence complexity, all of which accounted for 68.7% and 63.4% of observed variance, respectively. The favorable results of validation support the use of MBG in the field of research and medical practice.
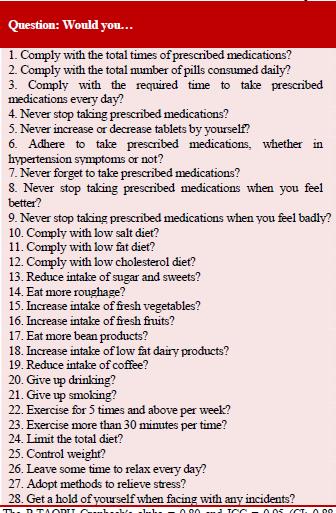
11. Treatment Adherence Questionnaire for Patients with Hypertension (TAQPH)
Ma et al.developed and tested the Treatment Adherence Questionnaire for Patients with Hypertension (TAQPH). The TAQPH consists of six subscales with 28 items. It is a measure dedicated for hypertensive patients allowing complete adherence evaluation including medication and lifestyle changes. The questionnaire was tested in a sample of 278 hypertensive patients in Guangdong Province of China, explaining 62.54% of the total variance in the data. Confirmative factor analysis supported a good overall fit of the six-factor model. The Cronbach’s alpha coefficient of the overall questionnaire was 0.86 and 0.82 for test-retest reliability. The authors concluded that the TAQPH can be applied for research and clinical purposes.

12. Adherence self-report questionnaire (ASRQ)
The Martin-Bayarre-Grau, a Spanish language 12- item questionnaire, was validated in Cuba in a population of 114 hypertensive patients. The Cronbach’s alpha coefficient of internal consistency was 0.889 for the sample. The second validation was performed in 142 patients with hypertension, with a Cronbach’s alpha value of 0.694. Validation results showed that the formulation of items was reasonable, clearly defined, and justified. The validation procedures allowed recognition of the existence of three factors: active adherence, autonomy in the face of treatment, and adherence complexity, all of which accounted for 68.7% and 63.4% of observed variance, respectively. The favorable results of validation support the use of MBG in the field of research and medical practice.
Conclusion:
There are various self-reported medication adherence tools. Some of them are disease specific and some of them are general. However, the main purpose of them all is to measure medication adherence of patients and ultimately improve their medication taking behavior thus improving quality of life of patients. Although the self-reported scale can give accurate result, but they are the most accessible and widely used measures. These tools had been developed in the one country at first following their culture, but when the same tool used by another country, cultural difference may arise, thus adaptation should be done by translating their own native language. Moving the Short Form 36-item questionnaire from the United States (source) to Japan (target) which would necessitate translation and cultural adaptation.
References:
- Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-care activities measure: results from 7 studies and a revised scale. Diabetes care. 2000 Jul 1;23(7):943-50.
- Hailu FB, Moen A, Hjortdahl P. Diabetes Self-Management Education (DSME) – Effect on Knowledge, Self-Care Behavior, and Self-Efficacy Among Type 2 Diabetes Patients in Ethiopia: A Controlled Clinical Trial. Diabetes Metab Syndr Obes. 2019;12:2489-2499
https://doi.org/10.2147/DMSO.S223123
- Beaton DE, Bombardier C, Guillemin F, Ferraz MB: Guidelines for the process of cross-cultural adaptation of self-report measures. Spine (Phila Pa 1976) 2000, 25: 3186–3191. 10.1097/00007632-200012150-00014
- Culig J, Leppée M. From Morisky to Hill-bone; self-reports scales for measuring adherence to medication. Collegium antropologicum. 2014 Mar 31;38(1):55-62.
- Kubica A, Kosobucka A, Michalski P, Fabiszak T, Felsmann M. Self-reported questionnaires for assessment adherence to treatment in patients with cardiovascular diseases. Medical Research Journal. 2017;2(4):115-22.
- https://www.michigancancer.org/bcccp/PDFs/WW2019/SelfEfficacyApprMedScale201901.pdf



.jpg)